
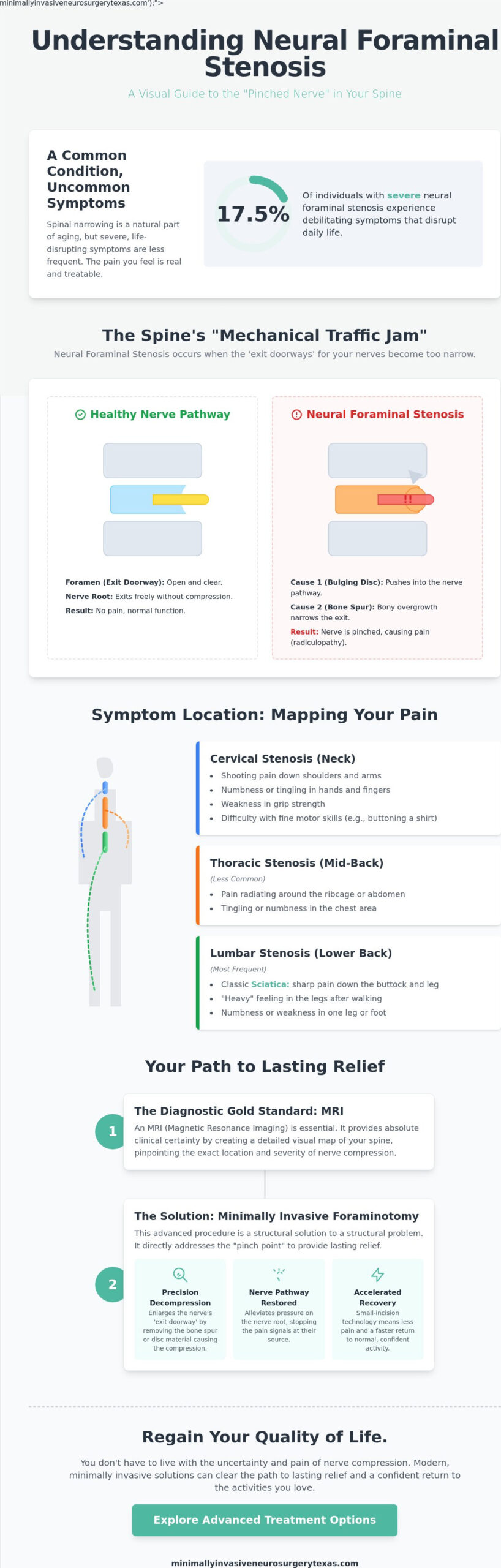
Research shows that while spinal narrowing is common as we age, only about 17.5% of individuals with severe neural foraminal stenosis actually experience the debilitating symptoms that disrupt daily life. If you are part of that percentage, you know that the shooting pain and sleepless nights feel like anything but a normal part of aging. It’s exhausting to live with the constant worry that your mobility is under threat or that permanent nerve damage is inevitable. You shouldn’t have to navigate this uncertainty alone.
We understand that your primary goal is to regain your quality of life without the fear of a long, painful recovery. You deserve to understand exactly why this mechanical traffic jam is happening in your spine and, more importantly, how modern medical innovation can clear the path to lasting relief. This guide explores the transition from conservative management to advanced, minimally invasive spine surgery. We will help you distinguish between mild cases and those requiring the precision of small-incision technology, providing a clear roadmap to return to normal activity with confidence.
Key Takeaways
- Learn the critical anatomical distinction between central canal narrowing and neural foraminal stenosis, and how these “exit doorways” impact your nerve health.
- Identify the hallmark signs of radiculopathy, including shooting pain and tingling, to better understand how the location of spinal narrowing dictates your symptoms.
- Discover how Degenerative Disc Disease and bone spurs act as mechanical culprits that shrink the space available for your nerves.
- Understand the diagnostic gold standard, including why an MRI is vital for visualizing nerve compression with absolute clinical certainty.
- Explore the benefits of a minimally invasive foraminotomy, a precision procedure designed to expand the nerve doorway and accelerate your return to normal activity.
Understanding Neural Foraminal Stenosis: The Anatomy of Spinal Narrowing
To understand why you feel radiating pain, you must first understand the architecture of your spine. Your spinal column is a masterwork of biological engineering, designed to protect the spinal cord while allowing nerves to branch out to the rest of your body. When this architecture changes due to age or injury, it often results in neural foraminal stenosis, a condition where the “exit doorways” for your nerves become dangerously narrow. This isn’t just a vague ache; it’s a structural issue that requires a structural solution.
The Foramen: Your Spinal Exit Ramp
The foramen is a small, bony opening between each pair of vertebrae. Think of it as a specialized exit ramp on a highway. While the main spinal canal carries the “highway” of the spinal cord, the foramen allows individual nerve roots to exit and travel to your arms, legs, and torso. The Anatomy of Spinal Narrowing explains that when these ramps become obstructed by bone spurs or bulging discs, the nerve root is compressed. Even a few millimeters of narrowing can create a significant mechanical pinch. This obstruction interrupts the flow of electrical signals, leading to the sharp, electric sensations that characterize nerve pain. Precision is our priority when identifying these pinch points.
It’s vital to distinguish this from central canal stenosis. Central stenosis involves the narrowing of the main channel that houses the spinal cord itself. In contrast, neural foraminal stenosis specifically targets the nerve roots at their point of departure. While central stenosis can cause widespread weakness or balance issues, foraminal stenosis typically results in symptoms that follow a very specific path down a single limb. We categorize this condition based on its location:
- Cervical: Located in the neck, affecting the shoulders, arms, and hands.
- Thoracic: Located in the mid-back, which is less common but can cause pain around the ribcage.
- Lumbar: The most frequent site, located in the lower back and causing sciatica in the legs.
Unilateral vs. Bilateral Stenosis
Most patients present with unilateral stenosis, meaning the narrowing only affects one side of the vertebrae. This explains why you might feel intense pain in your left leg while your right leg remains perfectly fine. Bilateral stenosis occurs when both the left and right exit ramps at a specific spinal level are narrowed. This often indicates more extensive spinal wear or a centrally bulging disc that has spread to both sides. Regardless of the presentation, the goal of modern intervention is to restore the space your nerves need to function without interference. Our approach focuses on decompressing these specific pathways to facilitate a swift return to normal activity.
Recognizing the Symptoms: How Stenosis Affects Your Daily Life
When a nerve is compressed within the spinal architecture, the resulting condition is known as radiculopathy. This isn’t a general backache. It is a specific, often searing sensation that travels along the path of the affected nerve. For those living with neural foraminal stenosis, symptoms often begin as a subtle nuisance before escalating into a constant presence that dictates every movement. The progression typically starts with intermittent discomfort during specific activities and can eventually evolve into a persistent “nerve fire” that refuses to subside, even at rest.
Citing authoritative clinical perspectives from institutions like Johns Hopkins on Diagnosis and Conservative Management highlights that while many individuals show spinal narrowing on imaging, the clinical experience of pain is what necessitates intervention. We focus on the functional impact of these symptoms to determine the most effective path forward for each patient.
Cervical vs. Lumbar Symptom Mapping
The location of the narrowing dictates exactly where you feel the impact. In the cervical spine, stenosis often sends “electric” shocks down the arm and into the fingertips. You might notice a sudden loss of grip strength or difficulty with fine motor tasks like buttoning a shirt. Lumbar stenosis, occurring in the lower back, is the primary driver of sciatica. This manifests as a sharp pain radiating through the buttocks and down the leg, often accompanied by a sensation of “heavy” legs after walking short distances. While thoracic stenosis in the mid-back is rarer, it typically presents as a localized pain that wraps around the ribcage or chest wall.
The Impact on Mobility and Quality of Life
Chronic nerve pain is never just a physical burden; it carries a heavy emotional toll. Sleep deprivation becomes a common reality as patients struggle to find a position that doesn’t trigger a pinch. Over time, many people subconsciously change how they move. You might find yourself leaning forward while walking to “make room” for the nerve or developing a slight limp to avoid putting pressure on a specific side. At Minimally Invasive Neurosurgery of Texas, our primary objective is to stop this cycle of decline and facilitate a swift return to normal activity through precise, high-tech solutions.
While most cases of neural foraminal stenosis develop gradually, certain “red flag” symptoms require an immediate neurosurgical evaluation. If you experience a sudden loss of bowel or bladder control, profound weakness in a limb, or numbness in the groin area, seek medical attention right away. These signs may indicate severe nerve compression that requires urgent decompression to prevent permanent damage. If your symptoms are persistent but less acute, a consultation with a specialist can help you understand your options for spine surgery that prioritizes your long-term mobility.
What Causes Neural Foraminal Narrowing? Identifying the Culprits
Understanding the origin of your pain is the first step toward reclaiming your mobility. While the symptoms of neural foraminal stenosis often feel like a sudden intrusion, the underlying causes are usually rooted in the mechanical evolution of the spine. When the structural components of your back change, the space available for nerve roots inevitably shrinks. This isn’t a condition that typically reverses on its own because the triggers are physical obstructions within the spinal architecture that don’t simply disappear with rest.
Several distinct factors contribute to this narrowing. Degenerative Disc Disease (DDD) is a primary culprit. As we age, the intervertebral discs lose hydration and “settle,” which brings the vertebrae closer together and reduces the height of the foraminal opening. In response to this instability, the body often produces bone spurs, or osteophytes. While these are intended to stabilize the joint, they frequently grow into the foramen and physically reduce the volume available for the nerve. Additionally, herniated discs can “clog” the exit doorway with soft tissue, while spondylolisthesis, or vertebral slippage, can shear the space shut entirely. Research into What Causes Neural Foraminal Narrowing? confirms that these mechanical blockages are the root of radicular pain.
The Role of Aging and Wear-and-Tear
For most patients, this condition is a gradual, age-related process. Years of supporting your body’s weight and managing daily movements lead to natural wear. Certain occupations that involve repetitive heavy lifting or prolonged vibration can accelerate this narrowing. You should feel reassured that while aging is inevitable, the resulting pain is a treatable medical condition. We focus on identifying these specific wear patterns to develop a targeted plan for your recovery.
Acute vs. Chronic Narrowing
It’s helpful to distinguish between sudden onset and slow progression. Acute narrowing often follows a specific injury, such as a fall or a sudden strain that causes a disc to herniated immediately into the foramen. Chronic narrowing is more common and stems from long-term arthritis. This slow progression often leads to “moderate” classifications on MRI reports, which can be deceptive for patients in significant pain. Bone spurs physically reduce the foraminal volume by occupying the space meant for the nerve root. Because this is a mechanical “traffic jam,” severe cases require the precision of Minimally Invasive Neurosurgery to clear the path and facilitate a return to normal activity.
Diagnosis and Conservative Management: The Path to Relief
Your diagnostic journey begins with a clinical correlation between your reported pain and physical evidence. While symptoms often point directly to the source, we utilize a rigorous physical examination to confirm the exact nerve root involved. This process involves testing dermatomes, which are specific areas of skin sensitivity, and myotomes, the muscle groups controlled by individual nerves. By identifying weakness in a specific toe flexor or numbness along a precise line on the leg, we can accurately locate the mechanical pinch causing your neural foraminal stenosis.
Magnetic Resonance Imaging (MRI) remains the gold standard for confirming this diagnosis. Unlike standard X-rays that only show bone, an MRI provides high-resolution visualization of soft tissues, including the discs, ligaments, and the nerves themselves. This level of detail is essential. It allows a neurosurgeon to see exactly how much “doorway” space remains for the nerve and whether the obstruction is a soft disc herniation or a calcified bone spur. This distinction is critical for determining whether conservative care is likely to succeed or if a more direct intervention is necessary.
Navigating Your Diagnostic Imaging
Radiology reports often categorize stenosis as “mild,” “moderate,” or “severe.” These terms describe the physical narrowing seen on the scan, but they don’t always dictate the level of pain you feel. Some patients with moderate narrowing experience significant disability, while others with severe findings remain functional. Because imaging must always correlate with physical symptoms, we prioritize how the condition impacts your daily life over the report’s adjectives. If your imaging findings are complex or don’t seem to match your clinical experience, seeking a specialist’s second opinion is a vital step in ensuring an accurate treatment plan.
When Conservative Care Reaches Its Limit
Most patients begin their recovery with conservative first steps. This typically includes a combination of activity modification, non-steroidal anti-inflammatory drugs (NSAIDs), and targeted exercises. Epidural Steroid Injections (ESIs) also play a dual role; they provide temporary relief by reducing nerve inflammation and serve as a diagnostic tool to confirm we have identified the correct level of the spine. However, we generally follow a “6-week rule” for these therapies. If six weeks of dedicated conservative management fails to provide meaningful relief, it is time to explore advanced pathways.
Ignoring progressive neurological deficits is a risk you shouldn’t take. Symptoms like muscle wasting, persistent foot drop, or a loss of fine motor skills indicate that the nerve is under significant duress. In these cases, minimally invasive neurosurgery offers a sophisticated middle ground. It provides a precision-engineered solution that clears the foramen without the trauma associated with traditional open procedures. If you are ready to move beyond temporary fixes, a consultation for spine surgery can provide the clarity you need to facilitate a return to normal activity.
Advanced Minimally Invasive Treatments for Foraminal Stenosis
When conservative measures no longer provide the quality of life you deserve, modern neurosurgery offers a path to relief that prioritizes your recovery. The primary goal of intervention for neural foraminal stenosis is decompression. This means physically removing the mechanical obstruction, whether it is a bone spur or a herniated disc, to lift the pressure from the pinched nerve root. By clearing this “traffic jam,” we restore the nerve’s ability to transmit signals without pain or interruption.
Traditional spine surgery once required large incisions and significant muscle disruption. Today, we utilize the Minimally Invasive Foraminotomy to achieve the same goals through an incision often smaller than a postage stamp. This procedure focuses on expanding the “doorway” of the nerve exit. By using specialized dilators to tunnel through muscle rather than cutting it, we preserve the structural integrity of your back. For even greater precision, Endoscopic Spine Surgery allows us to use ultra-high-definition cameras to visualize the nerve root with unparalleled clarity. These advanced tools ensure that only the offending tissue is removed, leaving healthy structures untouched.
The benefits of the MINT approach are measurable and significant. Patients typically experience less blood loss and minimal muscle damage compared to older surgical methods. This precision leads to reduced post-operative discomfort and a significantly faster recovery timeline. Our focus is always on the most efficient pathway to facilitate a return to normal activity.
Precision Decompression: Foraminotomy and Laminotomy
The process of freeing a nerve involves removing a small, targeted piece of bone or ligament. To ensure absolute accuracy, we often incorporate robotic navigation and augmented reality systems, such as the Globus Excelsius. These high-tech hallmarks allow for real-time tracking of surgical instruments with sub-millimeter precision. Because these techniques are so refined, many decompression procedures in Plano and Lewisville are performed on an outpatient basis. This allows you to begin your recovery in the comfort of your own home on the same day as your procedure.
Is Fusion Necessary? Exploring Modern Alternatives
A common concern for patients is whether they will require a permanent stabilization of the spine. We always explore the least invasive option that provides a lasting result. While some cases of instability may require a minimally invasive spinal fusion, many patients are candidates for motion-preserving alternatives. For those with cervical issues, artificial disc replacement can be an excellent way to treat stenosis while maintaining the natural flexibility of the neck. Our patient-centered philosophy ensures that your surgical plan is as unique as your anatomy, focusing on long-term mobility and the relief of suffering.
Reclaiming Your Mobility and Quality of Life
Living with the radiating pain of neural foraminal stenosis doesn’t have to be your permanent reality. You’ve learned that this condition is fundamentally a mechanical issue where the nerve’s exit doorway becomes obstructed by physical changes in the spine. Whether the cause is a bone spur or a degenerative disc, the solution lies in precision decompression. By identifying the exact source of your discomfort through advanced imaging and clinical correlation, you can move away from temporary fixes and toward a definitive resolution.
Board-certified neurosurgeon Dr. Scott Kutz and our team specialize in the most advanced pathways to relief. We are specialists in robotic-assisted and endoscopic spine surgery, utilizing high-tech systems to ensure maximum accuracy with minimal physical impact. With convenient locations in Plano and Lewisville, we provide the specialized, boutique care necessary for a swift recovery. The path forward is clear. Schedule a consultation with Dr. Scott Kutz at Minimally Invasive Neurosurgery of Texas today.
It’s time to prioritize your health and begin your journey back to a pain-free life. We are dedicated to helping you facilitate a return to normal activity with confidence.
Frequently Asked Questions
Is neural foraminal stenosis a serious condition?
Neural foraminal stenosis is serious when it causes neurological deficits or chronic, debilitating pain. While many people have mild narrowing without symptoms, severe cases can lead to permanent nerve damage if the compression isn’t addressed. You should monitor for “red flag” symptoms like muscle weakness or a loss of sensation. Early intervention often prevents the progression of these issues and facilitates a return to normal activity.
Can foraminal stenosis be cured without surgery?
Conservative treatments like physical therapy and anti-inflammatory medications manage symptoms, but they don’t cure the underlying structural narrowing. These methods aim to reduce inflammation around the nerve root to provide temporary relief. If the narrowing is caused by bone spurs or significant disc settling, the mechanical obstruction remains. When conservative care fails to improve your quality of life, minimally invasive options become the next logical step.
What is the difference between spinal stenosis and foraminal stenosis?
The primary difference lies in the location of the narrowing within the spinal architecture. Spinal stenosis typically refers to the narrowing of the central canal where the spinal cord resides. In contrast, neural foraminal stenosis specifically affects the “exit doorways” where individual nerve roots leave the spinal column. While central stenosis often causes widespread leg weakness, foraminal stenosis usually results in radiating pain down one specific limb.
How long can you live with neural foraminal stenosis before needing intervention?
You can live with this condition indefinitely as long as your symptoms are manageable and there’s no evidence of progressive nerve damage. Many patients manage mild narrowing for years using activity modification and periodic treatments. However, if you experience muscle wasting, constant numbness, or pain that prevents sleep, intervention is necessary. We generally recommend a surgical consultation if conservative management hasn’t provided relief within six weeks.
What exercises should I avoid if I have foraminal narrowing?
You should avoid high-impact activities and exercises that involve heavy lifting or extreme spinal extension. Movements that force the back into an arched position can further compress the foramen and pinch the nerve root. Avoid running on hard surfaces or performing heavy squats and overhead presses. Instead, focus on low-impact movements that stabilize the core without placing undue stress on the narrowed exit points of your spine.
What happens if neural foraminal stenosis is left untreated?
Leaving severe neural foraminal stenosis untreated can lead to chronic pain and permanent neurological deficits. Over time, constant pressure on the nerve root may cause muscle atrophy, persistent weakness, and a loss of coordination in the affected limb. In some cases, the nerve may lose its ability to transmit signals entirely. Early diagnosis and a precision-engineered treatment plan are essential to protect your long-term mobility and health.
Can a herniated disc cause foraminal stenosis?
A herniated disc is a frequent cause of acute foraminal narrowing. When the soft inner material of a disc protrudes into the foramen, it physically “clogs” the space intended for the nerve root. This creates immediate pressure and chemical irritation, leading to sharp, radiating pain. While some herniations resorb over time, others require minimally invasive neurosurgery to remove the offending tissue and restore the nerve’s pathway safely.
How successful is minimally invasive surgery for foraminal stenosis?
Minimally invasive procedures have exceptionally high success rates for relieving the symptoms of spinal narrowing. Because we use high-definition cameras and robotic guidance, the decompression is extremely precise. Patients benefit from smaller incisions, less muscle trauma, and significantly faster recovery times compared to traditional open surgery. Most individuals return to their daily routines much sooner, enjoying a long-term reduction in pain and a restored quality of life.

