What if the alphanumeric code on your MRI report isn’t just medical jargon, but a precise GPS coordinate for your recovery? It’s common to feel a surge of anxiety when you see terms like L4-L5 or C5-C6 for the first time. You’re likely searching for answers about your chronic pain, yet the technical language often feels like a barrier between you and the relief you deserve. Understanding vertebrae numbers is the first step in demystifying your diagnosis and reclaiming control over your health journey.
We agree that navigating spinal health should be transparent, not overwhelming. This guide will teach you exactly how your spine is organized and what those specific designations mean for your mobility and future treatment options. Whether you’re consulting with a specialist in Plano or Lewisville, having this knowledge allows for a more productive dialogue about your care. We’ll preview the spinal map, explain why certain levels are more prone to injury, and explore how 2026 advancements in minimally invasive neurosurgery and artificial disc replacement are providing faster, more precise paths for a return to normal activity.
Key Takeaways
- Master the foundational structure of the human spinal column, including the 33 vertebrae that safeguard your central nervous system.
- Decode the medical shorthand used in your MRI results by learning how vertebrae numbers and letters categorize the three primary spinal regions.
- Clarify the concept of “spinal levels” to understand why conditions like herniated discs are often diagnosed between two specific vertebrae.
- Explore the anatomy of a single vertebra to see how its components support your weight while creating a secure canal for your nerves.
- Learn how advanced robotic platforms like Globus Excelsius enable precision-targeted minimally invasive neurosurgery for a faster return to normal activity.
The Human Spinal Column: An Overview of the 33 Vertebrae
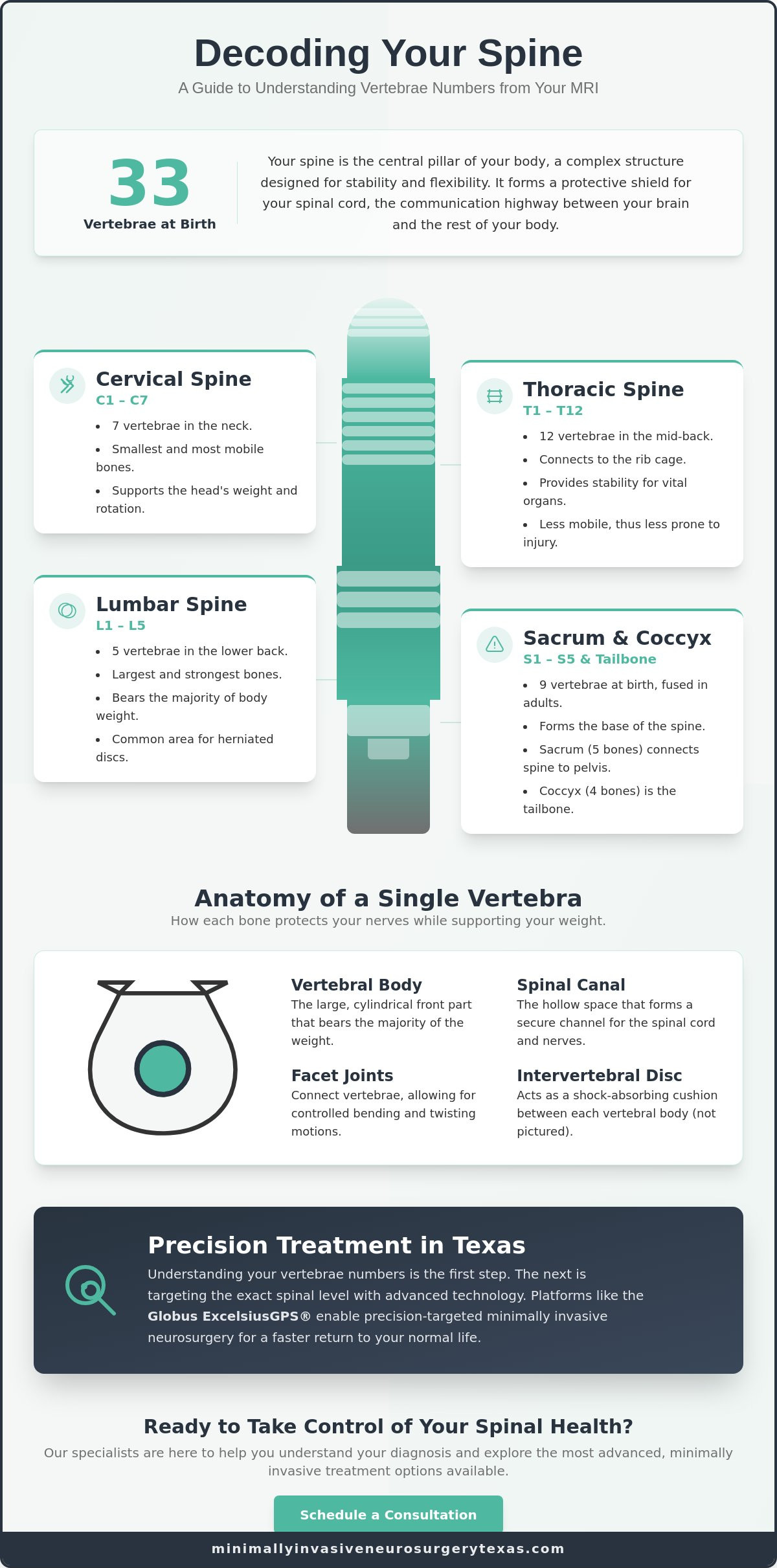
Your spine is the central pillar of your physical existence. It serves as the primary support structure for your weight while acting as a rigid shield for your central nervous system. When we discuss The Human Spinal Column: An Overview of the 33 Vertebrae, we are looking at a complex biological architecture designed for both stability and flexibility. At birth, every human typically has 33 individual bones. These vertebrae numbers are categorized into five distinct regions, each serving a unique mechanical purpose. Precision in identifying these levels is the cornerstone of modern spinal care and diagnostic accuracy.
As you grow, the “functional” number of bones changes. In an adult, the lower segments of the spine undergo a natural fusion process. This means that while you still have the same biological material, the sacrum and coccyx become solid structures. This evolution is vital for pelvic stability and weight distribution. The spinal cord, your body’s communication highway, runs directly through the hollow center of these stacked vertebrae. Any misalignment or injury to these numbered channels can disrupt signals sent from your brain to your limbs. This is why accurately identifying vertebrae numbers on an MRI is so vital for your surgeon to determine the best path forward.
The Five Regions of Your Spine
The spine is divided into three primary mobile sections and two fused sections. These are generally labeled by their region and a corresponding number:
- Cervical Spine (Neck): Consists of the C1 through C7 vertebrae. These are the smallest and most mobile bones; they allow you to tilt and rotate your head with ease.
- Thoracic Spine (Mid-back): Encompasses the T1 through T12 vertebrae. These connect to your ribs and provide essential stability for your chest and internal organs.
- Lumbar Spine (Lower back): Includes the L1 through L5 vertebrae. These are the largest bones because they bear the majority of your body weight.
Most patients seeking back surgery or minimally invasive neurosurgery find that their issues originate in the high-pressure lumbar region, where the weight of the torso meets the mobile base of the spine.
The Base: Sacrum and Coccyx
The foundation of your spine consists of the sacrum and the coccyx. The sacrum is a shield-shaped bone made of five fused segments, labeled S1 through S5. It fits between the hip bones to stabilize the pelvis and transfer weight to the lower limbs. Below that, the coccyx, or tailbone, consists of four small fused segments. Understanding the S1 region is particularly important for patients. Because the S1 segment sits directly below the L5 vertebra, pain originating here often mimics lumbar issues like sciatica. Distinguishing between a lumbar problem and a sacral issue is a critical step in planning effective spine surgery. It ensures that the treatment targets the exact source of the distress rather than just the symptoms, paving the way for a successful recovery.
Decoding the Regions: Cervical, Thoracic, and Lumbar Vertebrae Numbers
The shorthand used in medical records isn’t designed to be cryptic. It’s a standardized naming convention that uses the first letter of the spinal region followed by a specific number. This system ensures that every healthcare provider, from your primary doctor to your neurosurgeon, is looking at the same map. Understanding these vertebrae numbers allows you to pinpoint the exact location of your symptoms and understand why certain movements trigger pain. While the Anatomy of a Single Vertebra provides the structural blueprint, the way these bones are grouped determines how your body moves and where it’s most vulnerable.
The cervical spine, labeled C1 through C7, supports the weight of your head and facilitates a wide range of rotation. Below it, the thoracic spine (T1-T12) acts as a rigid anchor for your rib cage. These mid-back vertebrae are less mobile, which protects your internal organs but also makes them less prone to the wear and tear seen in other areas. The lumbar spine, consisting of the L1 through L5 vertebrae, serves as the heavy lifter of the body. These bones bear the majority of your body weight and provide the flexibility needed for bending and lifting. Because the lumbar region handles such significant loads, it’s often the first area to show signs of age-related degeneration.
The High-Traffic Zones: C5-C6 and L4-L5
Certain levels of the spine are more susceptible to injury due to the intense mechanical loads they carry. The C5-C6 level is frequently the site of disc herniations because it’s a primary pivot point for neck movement. This makes it the most common site for neck disk replacement in 2026. Similarly, the L4-L5 and L5-S1 levels in the lower back are the epicenter of most pathology because they support the entire weight of the torso. These specific joints wear out faster because they sit at the base of highly mobile regions where mechanical stress is most concentrated.
The Transition Points
Transition points occur where the spine changes its shape or function. The cervicothoracic junction (C7-T1) is where the mobile neck meets the rigid mid-back, creating a unique stress profile. Another critical area is the thoracolumbar junction (T12-L1), where the spine switches from the stability of the rib-anchored thoracic region to the mobility of the lumbar region. These transition points are often the focus of minimally invasive spinal fusion Texas patients require when instability occurs at these mechanical intersections. If you’re experiencing localized pain at these junctions, a consultation for minimally invasive neurosurgery can help determine if precision intervention is necessary to restore your quality of life.
Anatomy of a Single Vertebra: Why the Components Matter
While our previous discussion focused on Decoding the Regions: Cervical, Thoracic, and Lumbar Vertebrae Numbers, understanding the internal architecture of a single bone is just as vital for your recovery. Each of the 33 vertebrae is a specialized unit designed to balance weight and protect delicate neural tissue. The front of the bone consists of the vertebral body, a thick, cylinder-shaped mass that acts as the primary weight-bearer. Behind this body lies the vertebral arch, a bony ring that creates a protective tunnel for your spinal cord. When these components are aligned correctly, they provide a stable foundation for your daily activities.
Movement is made possible by the facet joints and intervertebral discs. Facet joints are small, cartilage-lined hinges that link the vertebrae together, allowing you to twist and bend without losing stability. Between every numbered level, you’ll find an intervertebral disc. These act as high-tech shock absorbers, preventing the bones from grinding against each other. If a disc fails at a specific level, it can lead to the need for an artificial disc replacement to restore natural motion. Precision in identifying these vertebrae numbers is essential because each component’s health directly impacts the stability of the entire column.
The Posterior Elements: Lamina and Spinous Process
The back of your vertebra features the spinous process, which are the visible bumps you feel when you run your hand down your back. Just beneath these lies the lamina, a flat plate of bone that serves as the “roof” of your spinal canal. In traditional surgery, this roof was often removed to relieve pressure. However, modern endoscopic spine surgery and other minimally invasive spine surgery techniques now allow surgeons to access the canal while sparing these vital posterior structures. This preservation leads to less trauma and a significantly faster return to normal activity.
The Neural Foramen: The Nerve Exit Ramps
At every vertebral level, there are side openings called the neural foramen. These function as exit ramps where nerve roots leave the spinal canal to travel to your arms or legs. There is a direct relationship between the numbered vertebra and the nerve root that exits there. For instance, a nerve exiting near the L4-L5 level controls specific muscles in your leg. When “foraminal stenosis” occurs, these ramps become narrow, pinching the nerve and causing radiating pain. Accurate diagnosis of these vertebrae numbers ensures that your surgeon can target the exact foramen causing your distress, providing the relief you’ve been seeking through specialized back surgery.
Reading Your MRI: What Vertebrae Numbers Mean for Your Diagnosis
Receiving an MRI report can feel like reading a coded message. You’ll often see clinicians refer to “levels” such as L4-L5 or C5-C6 rather than a single bone. This is because the spine functions through the “motion segment,” which is the smallest functional unit of your back. A motion segment consists of two adjacent vertebrae, the intervertebral disc between them, and the two facet joints that connect them. When your doctor reviews your vertebrae numbers, they aren’t just looking at the bones; they’re evaluating how this entire unit performs under pressure. If a report mentions a “protrusion at L4-L5,” it means the disc between those two specific bones is bulging into the spinal canal.
Understanding these levels helps explain why a problem in your lower back can cause pain in your toes. For example, the L5 nerve root exits near the L5 vertebra and travels all the way down the leg to the big toe. If there’s narrowing, or stenosis, at this specific numbered level, you might experience the classic shooting pain known as sciatica. By identifying the exact vertebrae numbers involved, your surgeon can determine if endoscopic spine surgery or another targeted back surgery is the most effective way to decompress the nerve and restore your mobility.
Mapping Your Symptoms to Vertebrae Numbers
You can often correlate your physical sensations with the data on your diagnostic imaging. This mental checklist helps you communicate more effectively with your specialist:
- C5-C6: Often results in weakness in the biceps and pain or numbness radiating into the thumb side of the hand.
- L4-L5: Frequently causes weakness when lifting the big toe or “foot drop,” along with pain across the top of the foot.
- L5-S1: Typically involves the Achilles reflex and causes pain or numbness along the outer edge of the foot.
If your symptoms align with these patterns, it’s a strong indicator of which motion segment requires clinical attention.
When “Failed” Fusion Happens at a Level
In some cases, a previous surgical site may not heal as intended, or the stress may shift to an adjacent level. This is often seen at the transition between the lumbar spine and the sacrum. Patients might experience symptoms of failed si joint fusion at the S1 level, which can include persistent localized pain or instability. Surgeons in Plano and Lewisville also watch for “adjacent segment disease,” where the vertebrae directly above or below a fused level begin to wear out prematurely. If you’re concerned about recurring pain after a previous procedure, a consultation for minimally invasive neurosurgery can provide clarity on your current spinal health and the most advanced options for revision.
Precision Treatment in Texas: Targeting Specific Spinal Levels
The anatomical map we’ve explored is the foundation for every surgical plan at our practice. Dr. Scott Kutz utilizes these precise vertebrae numbers to design a recovery path that is as unique as your own biology. By identifying the exact motion segment causing your distress, he can perform minimally invasive neurosurgery with unparalleled accuracy. This level-specific approach is enhanced by the Globus Excelsius robotic navigation platform. This technology allows our team to hit the exact numbered target with sub-millimeter precision, ensuring that the intervention is confined to the problematic area while leaving healthy tissue untouched.
The MINT philosophy centers on the idea of focused preservation. We believe in treating the specific level that requires attention while protecting the rest of your spinal column. When we pinpoint a level like L3-L4, it allows for significantly smaller incisions. These smaller openings mean less disruption to the surrounding muscles and ligaments, which translates directly to a faster recovery and a quicker return to normal activity. By focusing on the data provided by your vertebrae numbers, we move away from the invasive “open” surgeries of the past and toward a future of data-driven, precise healing.
Minimally Invasive Options for Numbered Levels
Modern surgical techniques are designed to address the specific needs of different spinal regions. For patients with issues in the cervical levels, we often prioritize artificial disc replacement over traditional fusion to maintain natural neck mobility. When performing lumbar spine surgery, we use the anatomical numbering to guide endoscopic access. This “keyhole” approach allows us to reach specific vertebrae through an opening no larger than a postage stamp. This method is particularly effective for decompressing nerves at a single, well-defined level without destabilizing the entire lower back.
Consulting a Specialist in Plano or Lewisville
Taking the next step toward relief starts with a comprehensive evaluation at our Plano or Lewisville facilities. We ask that you bring your recent MRI discs and formal reports to your first appointment. These documents are the blueprints we use to correlate your physical symptoms with your internal anatomy. Often, the question of what is back fusion surgery arises during these consultations. It’s important to understand that fusion isn’t a general solution, but a targeted conversation about stabilizing specific, numbered levels that have lost their structural integrity. For patients in North Texas ready to move past chronic pain, identifying the source at the vertebral level is the first step toward a successful clinical outcome.
Take Control of Your Spinal Health Journey
Navigating the complexities of spinal anatomy doesn’t have to be a source of anxiety. You now understand that vertebrae numbers are the key to a targeted, precise recovery plan rather than just confusing medical shorthand. By mastering the spinal map and learning how specific levels like L4-L5 or C5-C6 impact your mobility, you’re better prepared to advocate for your own health. Precision in diagnosis is the first step toward the relief of suffering and a successful clinical outcome.
Board-certified neurosurgeon Dr. Scott Kutz specializes in translating these anatomical details into actionable treatment plans. Utilizing advanced technology like the Globus Excelsius robotic navigation system, our practice focuses on minimally invasive techniques that prioritize your long-term stability. This high-tech approach ensures that we treat the exact source of your pain while facilitating a faster return to normal activity. Don’t let spinal confusion delay your progress toward a pain-free life. Schedule a Consultation with Dr. Scott Kutz in Plano or Lewisville today. Your journey toward lasting relief is built on a foundation of trust and expert care.
Frequently Asked Questions
How many vertebrae are in each part of the spine?
The human spine typically consists of 7 cervical, 12 thoracic, and 5 lumbar vertebrae, followed by the fused segments of the sacrum and coccyx. These 33 original bones provide the structural framework for your entire body. While the count remains consistent, the way these vertebrae numbers function changes as the lower segments fuse during adulthood. This organization allows for a sophisticated balance of mobility in your neck and lower back with rigid protection in your mid-back.
What is the most common vertebrae to have problems with?
The L4-L5 and L5-S1 levels in the lower back are the most frequent sites for clinical issues. These vertebrae bear the brunt of your body weight and facilitate significant bending and twisting. In the neck, the C5-C6 level is also a high-traffic zone for wear and tear. Because these specific joints handle intense mechanical stress, they’re the most common targets for back surgery or artificial disc replacement to restore quality of life.
What does it mean if my MRI says L4-L5 herniation?
An L4-L5 herniation indicates that the intervertebral disc located between your fourth and fifth lumbar vertebrae has shifted or ruptured. This specific motion segment is a vital pivot point for your lower body. When the disc material escapes its casing, it can compress the nearby L5 nerve root, leading to symptoms like leg pain or weakness. Identifying these precise vertebrae numbers allows your surgeon to plan a targeted decompression using minimally invasive techniques.
Can you live with a fused vertebra?
You can certainly live a full and active life with a fused vertebra. Spinal fusion is a proven method to eliminate painful motion at a specific, unstable segment. While the fused level no longer moves, the rest of your spine compensates to maintain your overall range of motion. Our goal with minimally invasive spine surgery is to stabilize the necessary level while preserving the health of the adjacent vertebrae to ensure long-term mobility.
Which vertebrae numbers are in the neck?
The cervical spine consists of seven vertebrae, labeled C1 through C7. C1, also known as the atlas, supports the skull, while C2, the axis, allows for head rotation. These seven bones are responsible for the incredible flexibility of your neck. If you experience pain radiating into your shoulders or arms, it’s often due to a nerve issue originating at one of these specific numbered levels in the cervical region.
What happens if a thoracic vertebra is misaligned?
Misalignment or injury in the thoracic region (T1-T12) often results in localized mid-back pain or discomfort that follows the path of the ribs. Because the thoracic vertebrae are anchored to the rib cage, they’re much more stable and less prone to herniation than the neck or lower back. However, issues here can still affect spinal cord health. Surgeons use precise imaging to address thoracic problems while maintaining the essential stability of the chest wall.
Is L5-S1 considered the lower back or the hip?
The L5-S1 level is technically the lumbosacral junction of the lower back, though pain here is frequently felt in the hip or buttock. This is the point where the mobile lumbar spine meets the stable sacrum. Because the nerves exiting at this level travel through the pelvic region, patients often mistake spinal nerve compression for a hip joint issue. A proper diagnostic workup distinguishes between these two areas to ensure the correct treatment.
How do surgeons find the right vertebrae number during surgery?
Surgeons utilize advanced intraoperative imaging and robotic navigation systems to identify the exact vertebral level during a procedure. Platforms like Globus Excelsius provide a digital map that correlates your preoperative MRI with your real-time anatomy. This high-tech guidance ensures that every instrument is placed with sub-millimeter precision. By verifying the vertebrae numbers before the first incision, we can perform minimally invasive neurosurgery with absolute certainty and safety.

