
Your cervical spine is a mechanical marvel that supports the full weight of your head while protecting the most vital electrical wiring in your body. Understanding your cervical spine anatomy is the first step toward reclaiming your quality of life. It’s common to feel overwhelmed when you look at an MRI report filled with technical jargon like “foraminal stenosis” or “C5-C6 disc bulge.” You aren’t alone in your frustration with vague diagnoses or the fear that a spinal issue might lead to a permanent injury.
We believe that an informed patient is a confident patient. This guide will help you identify the specific structures from C1 to C7 mentioned in your medical records and clarify the difference between bone and nerve pain. With success rates for cervical fusion surgery reaching 85 to 95 percent according to Sidecar Health, relief is achievable. We’ll explore the architecture of your neck, prepare you for a neurosurgical consultation, and discuss why modern advancements like the 2026 Medicare shift toward outpatient procedures are making recovery faster than ever. It’s time to move past the confusion and get back to life.
Key Takeaways
- Master the fundamental roles of the seven vertebrae (C1-C7) in supporting your head and protecting the central nervous system’s information highway.
- Decode complex medical terminology in your imaging reports by learning the specific regions of cervical spine anatomy, from the Atlas to the subaxial spine.
- Differentiate between bone-related pain and nerve irritation by understanding the relationship between intervertebral discs and the vertebral foramen.
- Identify how clinical conditions like herniated discs or spinal stenosis disrupt your neck’s architecture and what targeted relief options are available.
- Learn how advanced imaging and a specialized neurosurgical approach can help you move past chronic pain and finally get back to life.
The Cervical Spine: The Specialized Architecture of the Neck
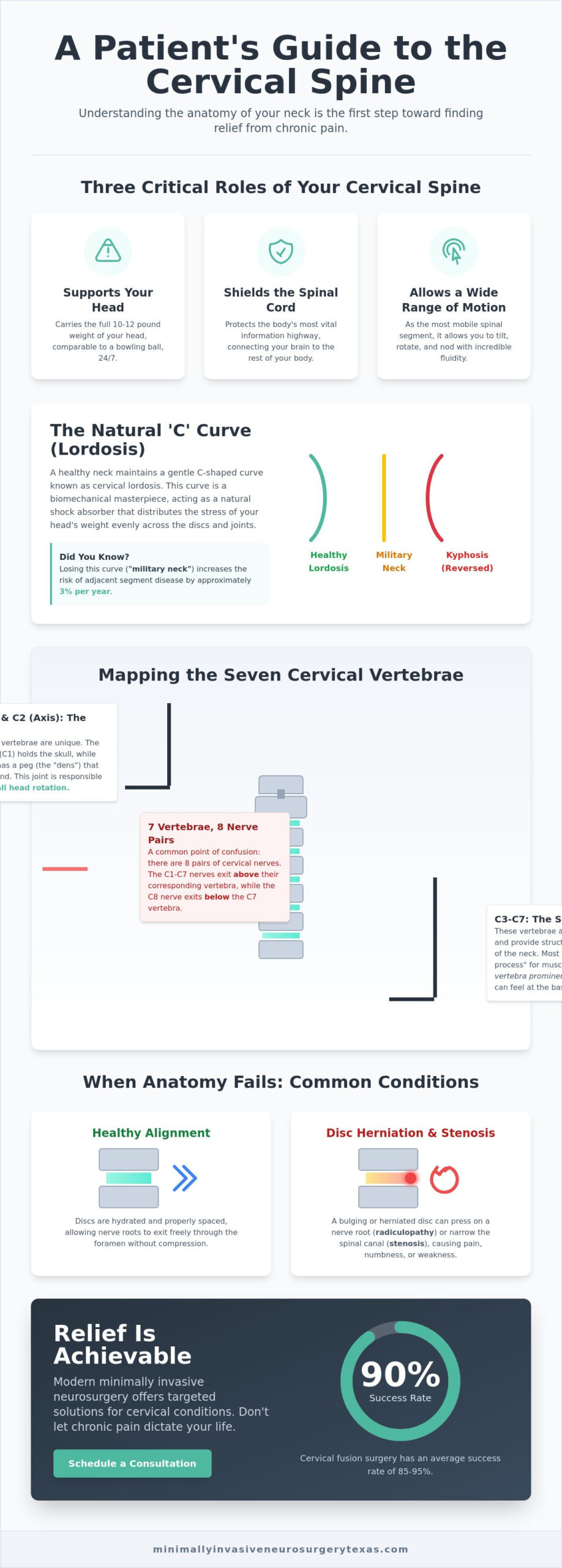
The cervical spine consists of seven specialized bones, known as Cervical vertebrae, labeled C1 through C7. These structures form the skeletal framework of your neck and serve as the foundation for every movement your head makes. As the most mobile segment of the entire vertebral column, this region allows you to tilt, rotate, and nod with incredible fluidness. At Minimally Invasive Neurosurgery of Texas, we view this delicate area through the lens of a High-Tech Healer. Precision is paramount because even a millimeter of displacement can impact your neurological health. Your cervical spine anatomy is designed to fulfill three critical roles: supporting the 10 to 12 pound weight of your head, shielding the spinal cord, and providing the widest range of motion in the human body.
Why the Cervical Spine is Unique
Cervical vertebrae are significantly smaller and more delicate than the heavy-duty segments found in your thoracic or lumbar spine. While your lower back is built for weight-bearing, your neck is engineered for agility. One of the most distinctive features of this region is the transverse foramen. These are small openings in the side of each vertebra that act as protective conduits for the vertebral arteries, which supply blood to your brain. Balancing a head that weighs as much as a bowling ball on such small structures requires a perfect harmony of bone and muscle. When this balance fails, chronic pain often follows. Understanding the nuances of your cervical spine anatomy helps you recognize why targeted, specialized care is necessary for this high-traffic area.
The Importance of the Lordotic Curve
A healthy neck doesn’t sit in a straight line; instead, it maintains a natural C-shaped curve called cervical lordosis. This curve acts as a shock absorber, distributing the mechanical stress of your head’s weight evenly across the spinal discs and joints. If you lose this curve due to injury or poor posture, you might develop “military neck,” where the spine becomes vertical. In more severe cases, the curve can reverse entirely, a condition known as kyphosis. Proper alignment is a primary goal during minimally invasive neurosurgery. Restoring this natural arc is often the key to relieving pressure on the nerves and helping patients get back to life. Without a proper lordotic curve, the risk of adjacent segment disease increases by approximately 3 percent per year. This makes anatomical precision a top priority for Dr. Scott Kutz and his team in Plano and Lewisville.
Mapping the Seven Cervical Vertebrae (C1 to C7)
Visualizing your neck as a simple column doesn’t do justice to its complexity. Your cervical spine anatomy is a sophisticated stack of seven vertebrae that interlock to create a secure conduit for the spinal cord. A common point of confusion for many patients is the nerve count. If you’ve ever wondered how many cervical vertebrae are there and how they relate to the nerves that branch from them, the answer reveals an important distinction: while there are seven cervical vertebrae, there are actually eight pairs of cervical spinal nerves. The first seven exit above their corresponding bone, while the eighth exits below the C7 vertebra. Each of these bones, except for C1, features a “bifid” spinous process. This small, split projection at the back of the vertebra acts as a specialized attachment point for the deep muscles of the neck, ensuring stability during movement.
C1 and C2: The Specialized Pivot
The top two levels of your spine are unlike any other bones in your body. The C1 vertebra, known as the Atlas, is a ring-like structure that supports the weight of the skull. It lacks a traditional vertebral body, which allows it to cradle the occiput perfectly. Directly beneath it sits the C2 vertebra, or the Axis. The Axis features a unique vertical projection called the dens or odontoid process. This peg acts as a pivot point, allowing the Atlas to rotate around it. This specific joint is responsible for approximately 50 percent of all head rotation. Because this area is so critical for mobility, detailed imaging is essential to understand the Anatomy of the Cervical Vertebrae when diagnosing upper neck pain.
C3 through C7: The Subaxial Spine
As we move down the neck, the vertebrae change shape to accommodate more weight. The subaxial spine, comprising C3 through C7, provides the structural support needed for the base of the neck. C7 is particularly easy to identify. It is known as the vertebra prominens because of its long, non-bifid spinous process that creates the noticeable bump at the base of your neck. In clinical practice, we often see the most significant wear and tear at the C5-C6 and C6-C7 levels. These segments are the “workhorses” of the neck, absorbing the most mechanical stress during daily activities. If you are experiencing pain in these lower levels, a consultation with Minimally Invasive Neurosurgery of Texas can help determine if the structural integrity of these segments has been compromised.
When these seven bones are stacked correctly, they form the vertebral foramen. This is the central opening that, when aligned, creates the spinal canal. This bony tunnel is the primary defense for your spinal cord. Any shift in alignment or narrowing of this canal can lead to serious neurological symptoms. Precision in mapping these levels is why we utilize advanced diagnostic tools to ensure every treatment plan is tailored to your specific skeletal structure.
The Soft Tissue Network: Discs, Nerves, and the Spinal Cord
While the vertebrae provide the skeletal frame, the soft tissue network brings life and stability to your neck. The spinal cord is the central “information highway” housed safely within the vertebral foramen. Surrounding this delicate cord are the ligaments—the Anterior Longitudinal Ligament (ALL), Posterior Longitudinal Ligament (PLL), and the Ligamentum Flavum. These act as high-strength “straps” that prevent excessive movement and keep your spine stable. When we examine cervical spine anatomy, we look at how these tissues interact to protect your neurological function. Any disruption in this network, whether from a sudden injury or gradual wear, can compromise the signals traveling from your brain to the rest of your body.
The Intervertebral Discs as Shock Absorbers
Intervertebral discs are the essential shock absorbers of the neck. Each disc consists of a tough outer ring called the annulus fibrosus and a jelly-like center known as the nucleus pulposus. These discs provide the necessary height for nerve roots to exit and the flexibility to turn your head without bone-on-bone friction. As we age, these discs lose hydration, leading to degenerative disc disease. It is a biological challenge because spinal discs have no blood supply, making self-repair difficult for the body to manage alone. This lack of nutrient flow is why a Comprehensive Guide to Cervical Spine Anatomy is vital for understanding why disc issues often require specialized intervention to resolve. When a disc loses its height, the space for your nerves shrinks, often leading to the “pinched” sensations that bring patients into our clinic.
The Cervical Nerve Map (C1-C8)
The cervical nerve map is a precise grid that dictates your physical capabilities. There are eight pairs of cervical nerves, labeled C1 through C8. The upper nerves (C1-C4) primarily control the muscles of the head and neck, as well as the diaphragm for breathing. The lower nerves (C5-C8) form the brachial plexus, which is the electrical grid for your shoulders, arms, and hands. If you feel tingling or weakness, the location of the sensation is a roadmap to the source of the problem. For example, C6 provides sensation to the thumb, C7 controls the middle finger, and C8 powers the pinky finger. These nerves exit the spine through small windows called the intervertebral foramen. If a disc herniates or bone spurs grow into these windows, the resulting nerve irritation can cause radiating pain far from the actual neck. Precision in identifying these levels allows us to apply targeted treatments that help you get back to life.
Clinical Implications: When Cervical Anatomy Fails
When the intricate balance of your cervical spine anatomy is disrupted, the consequences range from localized stiffness to debilitating neurological deficits. A herniated disc occurs when the nucleus pulposus escapes through a tear in the annulus fibrosus and irritates a nearby nerve root. This specific failure often leads to radiculopathy, which is pain, numbness, or weakness that travels down the arm. In contrast, myelopathy refers to the compression of the spinal cord itself. This is a significantly more serious condition that can impact your balance, coordination, and even bowel or bladder function. Understanding these terms helps you move past the frustration of a vague “neck pain” diagnosis and toward a targeted recovery plan.
Stenosis is another common anatomical failure that patients encounter on MRI reports. Spinal stenosis refers to the narrowing of the central canal where the spinal cord resides. Foraminal stenosis occurs when the “exit doors” for individual nerves become too tight. Both conditions can result from the natural aging process or sudden trauma. When these spaces narrow, the pressure on neural structures increases, often requiring a specialist’s intervention to prevent long-term damage. Identifying whether your pain stems from a single nerve root or the central cord is the first step in determining the right surgical or non-surgical path.
Bone Spurs and Osteophytes
Your body is remarkably adaptive, but its attempts to heal can sometimes cause more problems. When the spine becomes unstable due to degenerative disc disease, the body creates extra bone called osteophytes, or bone spurs, to provide additional support. While these spurs are meant to stabilize the joint, they often grow into the spaces reserved for nerves or the vertebral arteries. This can lead to a specific set of symptoms, including dizziness, “pins and needles” in the hands, and a noticeable loss of fine motor skills. If you find it difficult to button a shirt or write clearly, bone spurs may be encroaching on your spinal canal.
The Impact of “Tech Neck” on Modern Anatomy
Modern lifestyle habits are actively reshaping human anatomy in ways that were rarely seen in previous generations. Prolonged forward head posture, commonly called “tech neck,” significantly increases the effective weight of your head on the cervical spine. While your head weighs 10 to 12 pounds in a neutral position, tilting it forward at a 60-degree angle can increase that load to 60 pounds. This constant strain accelerates wear on the C5-C6 and C6-C7 levels, leading to premature anatomical changes. At Minimally Invasive Neurosurgery of Texas, we specialize in identifying these structural shifts before they cause permanent nerve damage. If you’re struggling with persistent symptoms, it’s time to schedule a consultation for expert spine surgery and get back to life.
Precision Treatment for Cervical Disorders in Plano and Lewisville
Understanding your cervical spine anatomy is more than an academic exercise; it’s the foundation of a successful recovery. At Minimally Invasive Neurosurgery of Texas, Dr. Scott Kutz applies a High-Tech Healer philosophy to bridge the gap between complex diagnoses and life-changing relief. We don’t believe in the one-size-fits-all approach common in large hospital systems. Instead, we utilize advanced MRI and CT imaging to map the unique nuances of your vertebrae and nerve roots. This precision allows us to move beyond the limitations of traditional open surgery, which often involves large incisions and lengthy hospital stays. By focusing on the specific structure causing your symptoms, we help you get back to life with minimal disruption to your daily routine.
Minimally Invasive Spine Surgery (MISS) for the Neck
Modern technology has revolutionized how we address issues like foraminal stenosis. Through Minimally Invasive Spine Surgery (MISS), we can perform procedures such as a Posterior Cervical Foraminotomy. This technique involves clearing the “exit door” for a pinched nerve using specialized instruments and tiny incisions. Our surgeons utilize endoscopic systems that provide 4K clarity, allowing them to visualize your anatomy with greater detail than the naked eye. The benefits for the patient are clear and measurable. You can expect less post-operative pain, reduced blood loss, and a significantly faster return to work. Most of our patients are able to return home the same day or the morning after their procedure, reflecting the shift in 2026 toward outpatient excellence in spine care.
Artificial Disc Replacement (ADR) vs. Fusion
When a disc in the neck fails, patients often face a choice between a traditional fusion and Artificial Disc Replacement (ADR). While cervical fusion has a success rate between 85 and 95 percent, it permanently locks the vertebrae together. This lack of movement can lead to adjacent segment disease, a condition that affects the levels above or below the fusion at a rate of approximately 3 percent per year. ADR is a motion-preserving alternative that utilizes innovative technology to mimic the function of a natural disc. By maintaining your neck’s natural range of motion, ADR reduces the stress on surrounding segments and preserves your long-term spinal health. For patients weighing their options, our detailed overview of neck disk replacement in Plano and Lewisville covers costs, the latest FDA-approved devices, and candidacy criteria to help you make an informed decision. Our specialized boutique centers in Plano and Lewisville are equipped with the latest navigational systems to ensure perfect hardware placement. Schedule a consultation in Plano or Lewisville to see if ADR is right for you and take the first step toward a pain-free future.
Take the Next Step Toward Lasting Relief
A clear understanding of your cervical spine anatomy is the most powerful tool you have in your recovery journey. You’ve seen how the delicate balance of vertebrae, discs, and nerves from C1 to C8 governs your ability to move and feel. When this balance is disrupted by stenosis or a herniated disc, you need a team that prioritizes precision over traditional, invasive methods. Our practice is dedicated exclusively to spinal health and mobility; this ensures you receive specialized attention rather than generalized care.
Board-certified neurosurgeon Dr. Scott Kutz utilizes advanced technological systems like Globus Excelsius and Augmedics AR to navigate the intricate structures of your neck with absolute certainty. These innovations allow us to offer minimally invasive solutions that preserve your natural motion and speed up your recovery. You don’t have to navigate chronic pain or confusing medical jargon alone. We’re ready to help you find a clear path forward so you can finally get back to life. Request an Appointment with Dr. Scott Kutz at MINT and start your journey to wellness today.
Frequently Asked Questions
How many cervical vertebrae are there in the human neck?
There are seven cervical vertebrae in the human neck, labeled C1 through C7. These bones form the top portion of your spinal column and provide the essential support for your skull. While there are seven bones, it’s a unique fact of cervical spine anatomy that there are actually eight pairs of spinal nerves that exit through this region. This structural arrangement allows for the high degree of flexibility required for daily head movements.
What is the most common cervical vertebra to have a herniated disc?
The C5-C6 and C6-C7 levels are the most common sites for a herniated disc in the neck. These segments bear the greatest amount of mechanical stress and provide the most movement, making them highly susceptible to wear and tear. Degenerative changes at these levels account for a high percentage of radiculopathy cases. When a disc fails here, it often impacts the nerves controlling the thumb, middle finger, or pinky.
Is C7 part of the neck or the upper back?
C7 is the final segment of the neck, though it sits at the transition point to the upper back. It is known as the vertebra prominens because its spinous process is the most visible bone at the base of the neck. While it marks the beginning of the cervicothoracic junction, its anatomical features still classify it as a cervical vertebra. It plays a vital role in anchoring the muscles that support the head and shoulders.
What is the difference between a cervical nerve and a cervical vertebra?
A cervical vertebra is a bony structure that provides physical support, while a cervical nerve is the electrical wiring that carries signals between the brain and the body. The vertebrae create a protective canal for the spinal cord, and the nerves exit through small openings called foramina. If the bone or disc shifts, it can pinch the nerve, leading to pain or weakness. Understanding this distinction is key to diagnosing whether your pain is structural or neurological.
Can cervical spine anatomy cause headaches?
Yes, abnormalities in your cervical spine anatomy frequently lead to cervicogenic headaches. These headaches typically originate from issues in the C1, C2, or C3 levels, where the nerves communicate with the same pathways used by the head and face. Irritation of these upper cervical nerves can cause referred pain that feels like a dull ache or pressure behind the eyes and at the base of the skull.
What happens if the C1 or C2 vertebrae are misaligned?
Misalignment of the C1 (Atlas) or C2 (Axis) vertebrae can severely restrict your head’s range of motion and cause significant neurological distress. Since 50 percent of neck rotation occurs at this specific joint, any instability here can lead to chronic pain or dizziness. In severe cases, misalignment can interfere with the vertebral arteries that pass through the transverse foramen, potentially affecting blood flow to the brain.
How does an artificial disc replacement mimic natural cervical anatomy?
Artificial disc replacement (ADR) mimics natural anatomy by preserving the motion between two vertebrae. Unlike a fusion, which locks the bones together, an artificial disc uses a medical-grade sliding mechanism to allow for tilting and rotation. This technology maintains the natural height of the disc space and reduces the risk of adjacent segment disease. It is a modern solution designed to help patients get back to life with their full range of motion intact.
Why is the cervical spine more prone to injury than the thoracic spine?
The cervical spine is more prone to injury because it is the most mobile and least protected segment of the spine. Unlike the thoracic spine, which is reinforced by the rib cage, the neck relies entirely on muscles and ligaments for stability. This high mobility, combined with the 10 to 12 pound weight of the head, makes the cervical region highly vulnerable to sudden acceleration injuries like whiplash or chronic postural strain.

